The Overlooked Muscle Behind Chronic Lower Back Pain
By Shaun Menashe, LAc, MTOM, Dipl. O.M. | Golden Mean Acupuncture, Los Angeles
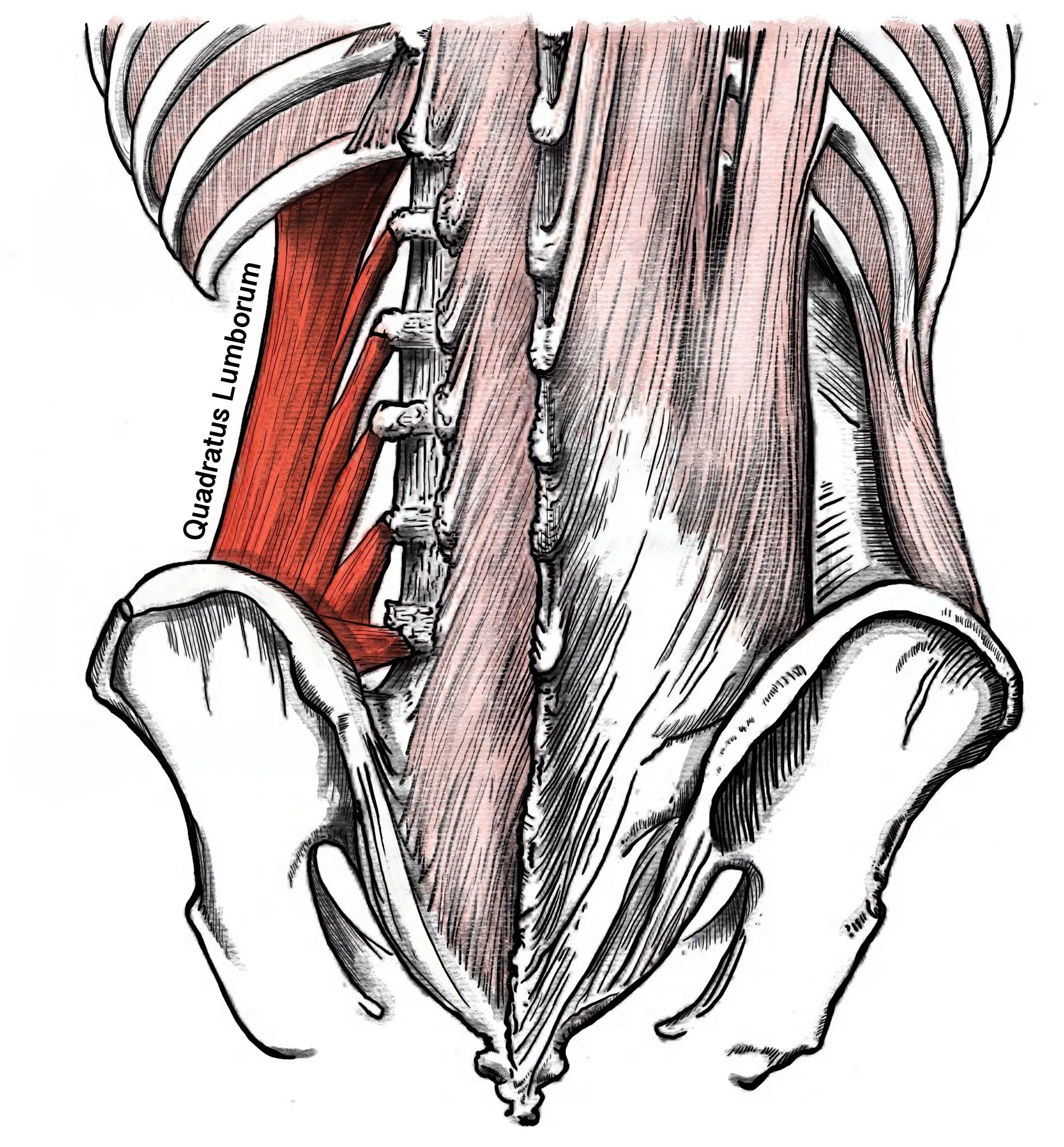
The quadratus lumborum, or QL, is a deep stabilizing muscle that connects the pelvis, lumbar spine, and twelfth rib. Although it rarely receives the same attention as discs, joints, or nerves, it plays a significant role in spinal stability, side bending, and force transfer through the lower back.
When the QL becomes chronically tight, overloaded, or compensating for weakness elsewhere, it can contribute to the diffuse, stubborn patterns of lower back pain that many patients describe. The pain tends to be constant rather than sharp, typically one-sided, and concentrated around the sacroiliac joint (the junction between the lower spine and the pelvis on either side). It is commonly aggravated by prolonged sitting, long car rides, and extended time at a desk, all positions that hold the hip in flexion and place the QL in a sustained shortened state.
Patients often describe feeling twisted or crooked. Hamstring tightness and gluteal tension are common accompanying findings, and on assessment it is not unusual to see scapular winging, one shoulder carried forward, and a visible preference for loading one leg over the other during functional movements like a squat. Reduced hip internal rotation on the symptomatic side is a frequent finding during assessment and often accompanies the broader compensation pattern. A visible stance preference is a common finding and often correlates with the side of QL overactivity, though the relationship varies between individuals and the direction of that preference cannot be assumed without assessment.
Understanding the QL's role helps fill an important gap between what imaging shows and what a patient actually experiences.
Key Takeaways
The quadratus lumborum (QL) is a deep stabilizing muscle connecting the pelvis, lumbar spine, and twelfth rib. It plays an important role in spinal stability, lateral flexion, and force transfer through the lower back, yet it is often overlooked in discussions of chronic back pain.
QL-related pain often presents as constant, one-sided discomfort around the sacroiliac region and may be aggravated by prolonged sitting, long car rides, or extended desk work. Patients frequently describe feeling twisted, compressed, or uneven rather than acutely injured.
The QL rarely functions in isolation. In clinical practice, reduced contribution from the gluteus medius is a common finding, and the QL often appears to compensate for pelvic stability during walking and other weight-bearing activities.
Acupuncture treatment may address this presentation through two complementary approaches: reducing tension in overactive tissue through trigger point needling and supporting neuromuscular activation in underperforming muscles through electroacupuncture (EA). These are distinct clinical goals that require different treatment strategies.
Patients benefit from an active treatment phase of three to five sessions, allowing each visit to build on the neurological and fascial changes initiated by the previous treatment. Long-term treatment frequency depends on movement patterns, workload, and recovery demands.
Lasting improvement typically requires more than temporary pain reduction. Addressing mobility restrictions, movement patterns, and load management helps create an environment where strengthening and corrective exercise can be more effective.
Built to Stabilize, Prone to Overload
The quadratus lumborum originates along the inner lip of the iliac crest (the broad wing of the pelvis you can feel with your hands on your hips) and the iliolumbar ligament. From there, its fibers travel upward in three distinct layers, attaching to the bony projections along the sides of the lumbar vertebrae and to the lower border of the twelfth rib (Bordoni and Varacallo, 2024). When both sides contract together, the muscle extends and stabilizes the lumbar spine. When one side contracts alone, it hikes the hip upward and bends the trunk toward the same side. It also anchors the twelfth rib during inhalation, giving the diaphragm a stable platform to contract against.
A QL under chronic tension compresses the twelfth rib downward toward the iliac crest, reducing the vertical space in the lumbar region and creating the sensation patients often describe as deep compression or being squeezed in the lower back.
The QL is also an integral component of the thoracolumbar fascia (the broad sheet of connective tissue spanning the posterior trunk) and participates in what anatomists describe as the lateral myofascial sling: a functional chain connecting the QL on one side with the gluteus medius and tensor fascia latae on the opposite side of the pelvis (Willard et al., 2012). When one link in that sling becomes dysfunctional, the whole system compensates.
When One Link Breaks
Understanding why the QL becomes overloaded requires looking at the broader network of muscles and connective tissue along the back of the body, what movement specialists often call the posterior chain. In clinical practice, a consistent finding is reduced contribution from the gluteus medius, the primary lateral hip stabilizer. When this occurs, the QL often appears to compensate for pelvic stability during gait and single-leg loading tasks, becoming chronically overactive.
A pelvis that has lost lateral stability sends effects through the kinematic chain. The hip joint loads unevenly, the thigh begins to rotate inward, and stress accumulates through the knee and foot. The shoulder girdle is drawn into the compensation as well, which is why patients with a chronically overloaded QL often present with one shoulder carried forward and visible asymmetry through the upper back.
A chronically shortened QL pulls the twelfth rib toward the iliac crest, reducing the space between the lower ribcage and pelvis and increasing load through the facet joints (the small paired joints along the back of the spine), causing vertical compression. This helps explain why QL-driven pain typically worsens with prolonged standing and improves briefly with lying down. It is worth noting that these relationships are rarely linear in practice. Whether gluteus medius inhibition precedes reduced hip internal rotation or the reverse is often impossible to determine from assessment alone. What these patterns share is that addressing any one element in isolation is unlikely to produce lasting change. A comprehensive approach that accounts for the full compensation pattern leads to lasting recovery.
Acupuncture and Functional Restoration
Treating this presentation effectively requires working on two problems simultaneously: releasing the tissue that is chronically overactive, and facilitating recruitment in the muscles that have become inhibited or under active, failing to fire at the level needed to support normal movement. These are distinct clinical goals that require different tools.
When a muscle like the QL develops myofascial trigger points, the sarcomeres (the contractile units within individual muscle fibers) become locked in a shortened state that local circulation cannot resolve on its own. Needling directly into these trigger points is thought to mechanically disrupt the contractile knot, with research documenting an associated increase in local blood flow and microcirculation to tissue that has been relatively oxygen-deprived (Shah et al., 2008).
The QL can be needled directly via two approaches. The first is through the lateral lumbar window, where needles are placed into the palpable trigger point bands along the muscle belly. The second targets the vertebral attachments using the Hua Tuo Jiaji points, a classical set of paravertebral points named for the Han dynasty physician Hua Tuo, located about half a thumb-width lateral to the midline at each lumbar vertebral level. Depending on the presentation, electroacupuncture (EA) may be applied between adjacent Jiaji points, delivering a gentle low-frequency electrical current that can further reduce muscle guarding and support neuromuscular regulation at the affected spinal levels. These two approaches address the muscle from its belly to its spinal origin and are used together rather than as standalone interventions.
Inhibition of the gluteus maximus and gluteus medius is addressed with electroacupuncture at GB30 (Huantiao, on the Gallbladder channel), located at the junction of the outer third and inner two-thirds of the distance between the greater trochanter (the bony prominence of the outer hip) and the base of the tailbone. GB30 overlies the gluteus maximus and lies in close proximity to the inferior gluteal nerve, the primary motor nerve for that muscle. In clinical experience, EA at GB30 with a low-frequency stimulation protocol consistently facilitates a motor response in the gluteus maximus and assists in reestablishing the neuromuscular pattern that allowed the QL to become overloaded in the first place. Trigger point assessment posterior to the greater trochanter is also performed, as gluteus medius tendinopathy is common in this presentation due to the chronic reduction in hip internal rotation and the resulting compressive load on the tendon at its insertion (Grimaldi et al., 2017). The gluteus medius is needled directly to address this alongside the lateral hip inhibition that drives compensatory QL overactivity.
Cupping is the final component of the protocol. Where needles address point-specific tissue, the negative pressure of cupping lifts the superficial and middle fascial layers away from the underlying musculature rather than compressing them, creating a decompressive effect along the lumbar region. A 2025 randomized controlled trial published in the Journal of Bodywork and Movement Therapies found that cupping produced immediate increases in lumbar range of motion and local temperature compared to placebo, though the authors noted effects were not significantly greater than placebo at the group level (Serrano-Carmona et al., 2025). A separate meta-analysis of six randomized controlled trials found cupping superior to control management for pain reduction in low back pain as measured by visual analog scale scores (Wang et al., 2017). Cupping is applied bilaterally along the lumbar paraspinals to address left-right asymmetry and restore fascial glide before reloading the area with movement.
For most presentations of this kind, an active treatment phase of roughly three to five sessions is appropriate, spaced close enough together that each session builds on the neurological and fascial changes initiated by the previous one. From there, maintenance frequency is determined by how the patient's movement patterns, workload, and recovery are holding.
The Longer Arc: Restoring the System, Not Just the Symptom
Pain relief is the entry point, not the destination. A QL that has been overloaded for months or years is embedded in a whole-body compensation pattern that includes hip mobility restriction, altered gait mechanics, and often some degree of foot and ankle stiffness that feeds tension back up the kinematic chain. Releasing the QL without addressing those downstream patterns is like resolving the loudest symptom without asking what produced it.
Acupuncture provides a graduated path through the tissue: each session restores a layer of fascial mobility and neuromuscular availability that makes the next layer of movement retraining possible. Patients typically notice that movements they could not access before, hip hinges, lateral band walks, single-leg balance work, become available after the locked tissue has been released. That sequencing matters: release the overactive tissue, facilitate the inhibited muscle, then support the transition into the movement work that creates durable change.
Ultimately, the work of understanding and supporting mechanics falls to the patient. The movement patterns ingrained by daily life are difficult to overcome without proper repatterning and counter-programming. It can seem like an unfair burden to place on someone in pain, but it is the reality of human biomechanics. When chronic tension and compensatory loading reduce the body's capacity to transmit force freely, movement retraining works against the tissue rather than with it. Restoring fascial mobility is the primer. Mobility training, weight-bearing progression, and corrective exercise are the paint, applied only to a suitable base. Patients who move directly into strengthening programs without first addressing underlying tissue restriction often plateau or regress. Acupuncture supports this preparatory layer by releasing restricted tissue and restoring neuromuscular availability. Coupled with a progressive return to loading and corrective movement, it creates the conditions in which reprogramming can actually take hold.
For patients in Echo Park and the surrounding neighborhoods dealing with back pain that has persisted through standard approaches, the assessment at Golden Mean Acupuncture begins with a functional question: which muscles are doing too much, which have stopped contributing, and what needs to change for the load to distribute correctly. That is almost always a more useful starting point than where the pain is located.
This article is intended for educational purposes only and does not constitute medical advice. The information presented here is not a substitute for professional medical consultation, diagnosis, or treatment. Always seek the guidance of a licensed healthcare provider before making any changes to your health protocol.
References
Bordoni B, Varacallo M. Anatomy, Abdomen and Pelvis, Quadratus Lumborum. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK535407/
Grimaldi A, Mellor R, Nicolson P, et al. Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain. British Journal of Sports Medicine. 2017;51(6):519-524. https://doi.org/10.1136/bjsports-2016-096175
Janda V. Muscles and motor control in cervicogenic disorders. In: Grant R, ed. Physical Therapy of the Cervical and Thoracic Spine. New York: Churchill Livingstone; 1994.
Serrano-Carmona JL, et al. Immediate effects of cupping therapy on pain, flexibility and temperature of the lumbar spine: a randomized controlled clinical trial. Journal of Bodywork and Movement Therapies. 2025;42:1025-1030. https://doi.org/10.1016/j.jbmt.2025.03.001
Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Archives of Physical Medicine and Rehabilitation. 2008;89(1):16-23. https://doi.org/10.1016/j.apmr.2007.10.018
Wang YT, Qi Y, Tang FY, et al. The effect of cupping therapy for low back pain: a meta-analysis based on existing randomized controlled trials. Journal of Back and Musculoskeletal Rehabilitation. 2017;30(6):1187-1195. https://doi.org/10.3233/BMR-169736
Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. Journal of Anatomy. 2012;221(6):507-536. https://doi.org/10.1111/j.1469-7580.2012.01511.x